The use of suprascapular nerve block injection for people with chronic shoulder pain within physiotherapy practice.
Neil Smith1 MRes, BSc
Dr Emma Salt2 PhD, MSc, BSc
Sandwell and West Birmingham Hospitals NHS Trust / Warwick Clinical Trials Unit.
University Hospitals of Derby and Burton NHS Foundation Trust
Introduction
Chronic shoulder pain is a major cause of disability; 20% of those affected still report shoulder pain at 1 year and 14% at 3 years.9,14,16 Chronic shoulder pain is most common in people aged 65 and over, affecting 1 in 5 people, with degenerative rotator cuff tears the most common chronic shoulder disorder in this age group.10 Local steroid injections are used in the management of chronic shoulder pain but only provide short-term benefit and regular repeat injections are not recommended.3,19
The major sensory nerve of the shoulder complex is the suprascapular nerve.2 The suprascapular nerve is a mixed motor / sensory nerve and supplies up to 70% of the sensory innervation to the shoulder complex, including the acromioclavicular joint, posterior joint capsule, rotator cuff tendons and subacromial bursa (Fig 1).2,8,17
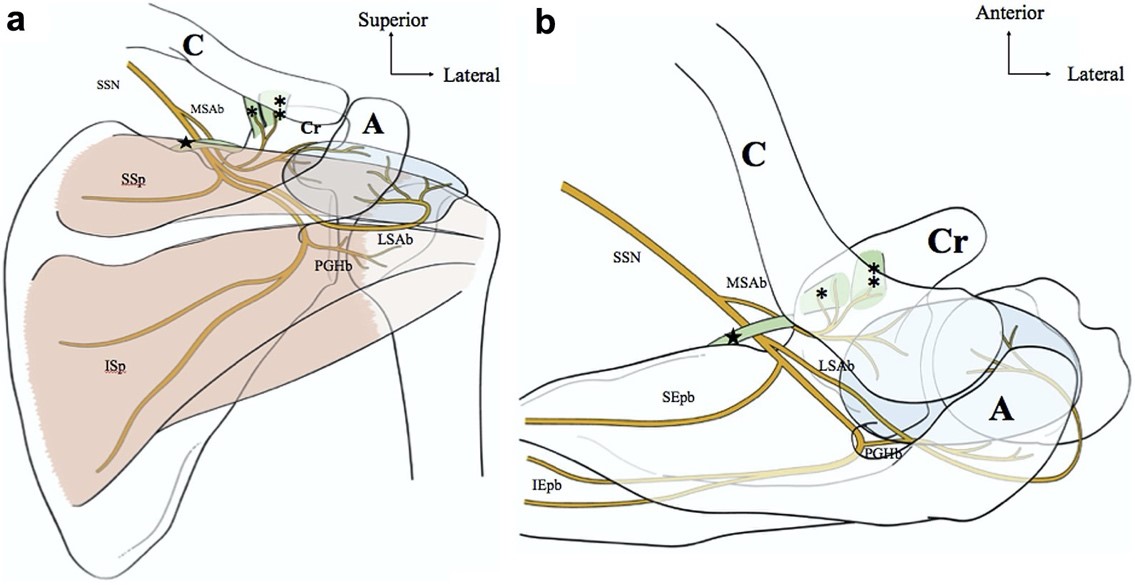
Fig 1 Schematic diagram of the distal suprascapular nerve (dSSN) and its sensory branches (a, posterior view; b, superior view). The SSN has 3 sensory branches: a medial subacromial branch proximal to the suprascapular notch, a lateral subacromial branch (LSAb) at the level of the suprascapular notch, and a posterior glenohumeral branch (PGHb) distal to the spinal glenoid notch. The subacromial branches provide bipolar innovation to the subacromial bursa (in blue); the medial subacromial branch (MSAb) also innervates the coracoclavicular ligaments (conoid (*) and trapezoid (**) ligament). The PGHb provide sensory innervation to the posterior glenohumeral capsule. A, acromion; C, clavicle; Cr, coracoid process; ISp, branch to infraspinatus muscle; SSp, branch to supraspinatus muscle. (Laumonerie P, et al, 2019).
Suprascapular nerve block injection was first described by Wertheim and Rovenstine (1941).18 Suprascapular nerve block injections are used for people with a range of chronic shoulder disorders4,5 and interest is growing in their use as a treatment option for people with chronic shoulder pain associated with rotator cuff tears and rotator cuff arthropathy.6,11,13
Suprascapular nerve block injection can be performed land-marked or using ultrasound, computer tomography and electromyography guidance, and using local anaesthetic alone or local anaesthetic combined with steroid.1,4,5,12 The optimal method of performing suprascapular nerve block injection is unknow.
Although suprascapular nerve block injections are recommended within UK shoulder pain guidelines, 7,15 and have shown promise in small clinical trials only low-level evidence exists to support its wider use.5
Physiotherapists use of suprascapular nerve block injection
A published 2019 survey of physiotherapists use of suprascapular nerve block injection revealed that from 121 physiotherapists that considered suprascapular nerve block injections for their patients, only 8 physiotherapists actually performed the injection themselves.11
Reasons why physiotherapists did not consider suprascapular nerve block injection in their patients included uncertainty about the benefits compared to other treatments, and uncertainty about long-term effectiveness and risks.11
The reasons why so few physiotherapists performed suprascapular nerve block injection themselves from the group that did consider them in their patients included lack of support from their work place, not part of shoulder care pathways, ability to refer to other services and omission of specific training on the intervention in injection training courses.11
During the APPN Upper Limb study day in January 2020 a brief survey was conducted on physiotherapists interest in performing suprascapular nerve block injection and being involved in future research in this area.
Although only 1 out of 120 people in the audience reported performing suprascapular nerve block injection in clinical practice, of those that completed the survey;
- 93% (40/43) reported a desire to perform suprascapular nerve block injections
- 67% (44/66) felt they required external additional training in order to perform them
- 87% (46/53) reported they would be interested in being involved in future research in this area.
The future of suprascapular nerve block injection within physiotherapy practice
Suprascapular nerve block injections are recommended within UK shoulder pain guidelines, 7,15 however only low-level evidence exists to support its use.5 If suprascapular nerve bock injections are found to be effective and can be delivered safely in a timely manner by advanced practice physiotherapists this could lead to improved patient outcomes and care pathways.
A high-quality, multi-centre randomised controlled trial, delivered within physiotherapy practice, is needed to determine the effectiveness of suprascapular nerve block injection in people chronic shoulder pain.
Prior to undertaking a randomised controlled trial research is needed to define best practice in suprascapular nerve block injection and in developing a training framework for physiotherapists to perform them.
Bibliography
- Bhayani S: Suprascapular nerve block injection (video) [Internet]. [cited 2020 Oct 20]. Available from: https://www.youtube.com/watch?v=nBS3N9efdWo
- Blum A, Lecocq S, Louis M, Wassel J, Moisei A, Teixeira P: The nerves around the shoulder. Eur J Radiol 82:2–16, 2013.
- Buchbinder R, Green S, Youd JM: Corticosteroid injections for shoulder pain. Cochrane Database Syst Rev [Internet] , 2003. Available from: http://doi.wiley.com/10.1002/14651858.CD004016
- Chan C, Peng P: Suprascapular nerve block: A narrative review. Reg Anaesth Pain Med 36:, 2011.
- Chang KV, Hung CY, Wu WT, Han DS, Yang R Sen, Lin CP: Comparison of the Effectiveness of Suprascapular Nerve Block With Physical Therapy, Placebo, and Intra-Articular Injection in Management of Chronic Shoulder Pain: A Meta-Analysis of Randomized Controlled Trials [Internet]. Arch. Phys. Med. Rehabil. Elsevier Ltd; 2016. Available from: http://dx.doi.org/10.1016/j.apmr.2015.11.009
- Hackney R, Cowling P, Ismail M, Javed M, Conaghan P, Kingsbury S: The Management of large and massive rotator cuff tears- Current trends amongst UK shoulder surgeons. Peertechz J Orthop Rheumatol [Internet] 3:005–0011, 2018. Available from: http://dx.doi.org/10.17352/ojor.000014
- Kulkarni R, Gibson J, Brownson P, Thomas M, Rangan A, Carr AJ, Rees JL: Subacromial shoulder pain. Shoulder Elb 7:135–43, 2015.
- Laumonerie P, Blasco L, Tibbo ME, Bonnevialle N, Labrousse M, Chaynes P, Mansat P: Sensory innervation of the subacromial bursa by the distal suprascapular nerve: a new description of its anatomic distribution. J shoulder Elb Surg Elsevier; 28:1788–94, 2019.
- Linsell L, Dawson J, Zondervan K, Rose P, Randall T, Fitzpatrick R, Carr A: Prevalence and incidence of adults consulting for shoulder conditions in UK primary care; patterns of diagnosis and referral. Rheumatology 45:215–21, 2006.
- Murphy RJ, Carr AJ: Shoulder Pain. BMJ Clin Evid [Internet] :1–37, 2010. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3217726/
- Salt E, Van Der Windt D, Chesterton L, McRobert C, Foster N: Physiotherapists’ use of Suprascapular Nerve Blocks: an online survey. Physiotherapy [Internet] The Chartered Society of Physiotherapy; 105:461–8, 2019. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0031940619300082
- Smith N, Liew Z, Johnson S, Ellard DR, Underwood M, Kearney RS: A systematic review of the methods and drugs used for performing suprascapular nerve block injections for the non-surgical management of chronic shoulder pain. (submitted to Br J Pain. Aug 2020)
- Tashjian RZ, Chalmers PN: What’s New in Shoulder and Elbow Surgery. J Bone Jt Surg – Am Vol Lippincott Williams and Wilkins; 101:1799–805, 2019.
- The World Health Organisation: WHO | International Classification of Diseases, 11th Revision (ICD-11). Int Classif Dis 11th Revis [Internet] World Health Organization; , 2019. Available from: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/1236923870
- Thomas M, Bidwai A, Rangan A, Rees JL, Brownson P, Tennent D, Connor C, Kulkarni R: BESS/BOA Patient Care Pathways Glenohumeral osteoarthritis. Shoulder Elb 8:203–14, 2016.
- Urwin M, Symmons D, Allison T, Brammah T, Busby H, Roxby M, Simmons A, Williams G: Estimating the burden of musculoskeletal disorders in the community : the comparative prevalence of symptoms at different anatomical sites , and the relation to social deprivation. Ann Rheum Dis 57:649–55, 1998.
- Vorster W, Lange CPE, Briët RJP, Labuschagne BCJ, du Toit DF, Muller CJF, de Beer JF: The sensory branch distribution of the suprascapular nerve: An anatomic study. J Shoulder Elb Surg 17:500–2, 2008.
- Wertheim, H.M. and Rovenstine EA: Suprascapular nerve block. Anesthesiology. J Am Soc Anesthesiol 2:541–5, 1941.
- NICE [Internet]. Clin. Knowl. Summ. 2017 [cited 2020 Oct 13]. Available from: https://cks.nice.org.uk/topics/shoulder-pain/management/rotator-cuff-disorders
Acknowledgements
Neil Smith is funded within a NHIR Pre-doctoral Clinical Academic Fellowship to undertake this research.